




You are now leaving the Evive Biotech website. Evive offers links to other third party websites that may be of interest to our website visitors. When you click on these links you will leave the Evive’s website and will be redirected to another site. These sites are not under the control of Evive Biotech. Click Continue to proceed or Cancel to go back.
Pipeline
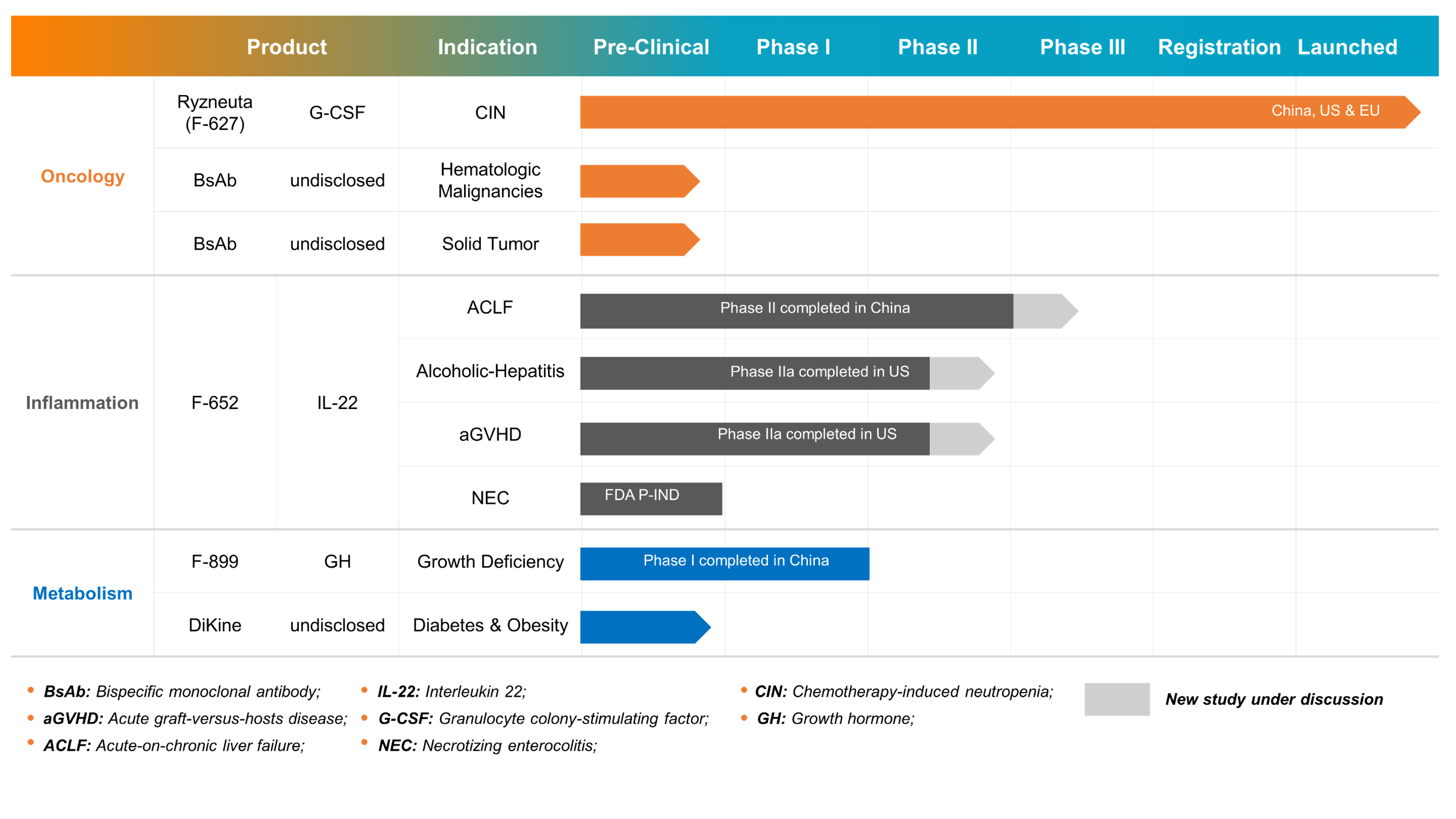
Building a Broad Product Pipeline with Worldwide Commercialization
Ryzneuta® [F-627]
<p>Ryzneuta® (F-627) is a novel, long-acting granulocyte colony-stimulating factor (G-CSF) intended to treat chemotherapy induced neutropenia (CIN) in patients with cancer.<br /> G-CSF binds to specific G-CSF receptors (G-CSFR) on the cell surface and influences the survival, proliferation, and differentiation of cells in the neutrophil lineage, from haemopoietic stem cell through mature neutrophil. Ryzneuta® is a recombinant fusion protein containing human G-CSF and the crystallizable fragment domain (Fc) of human immunoglobulin G2 (IgG2). It is expressed in and purified from Chinese hamster ovary (CHO) cell culture. Ryzneuta® exists as a homodimer, and it has an immunoglobulin like structure with a G-CSF molecule at each of the amino (N)-terminals. Ryzneuta® is a fully biodegradable long-lasting G-CSF-Fc protein that provides patients with all the benefits of new generation G-CSF products due to its unique dimeric fusion protein structure which does not require pegylation; additionally, Ryzneuta® has a good safety profile and a robust manufacturing process.</p>
- Chemotherapy Induced Neutropenia [CIN]
Neutropenia is a well-recognized condition that predisposes patients to bacterial and fungal infection; susceptibility to infection increases dramatically with severe neutropenia (absolute neutrophil count (ANC)<0.5 × 109/L). Cytotoxic chemotherapy agents target rapidly dividing cells, including myeloid progenitor cells. Therefore, patients with malignancies who are receiving chemotherapy are at risk of developing neutropenia. The degree of risk, as reflected by the incidence and duration of severe neutropenia, and the rate of febrile neutropenia (i.e., severe neutropenia with a coexistent fever), are substantially driven by the chemotherapy agents and doses used. Management of severe neutropenia in cancer patients receiving myelotoxic chemotherapy, remains a challenge in clinical practice since it can result in significant morbidity and/or mortality due to infectious complications, as well as chemotherapy dose reductions/delays, which may compromise treatment outcomes. Supportive care with recombinant human G-CSFs (rhGCSFs) has been very beneficial in reducing neutropenia and its complications in patients receiving myelotoxic chemotherapy. Patients receiving short-acting G-CSF products, such as filgrastim, require daily administrations during every chemotherapy cycle. F-627 was designed to evoke synergetic actions from the biological functions of both G-CSF and Fc moieties to elicit long-lasting actions which differentiates itself from other G-CSF products on pharmacokinetic/pharmacodynamic profiles as well as ultimate therapeutic efficacy.
F-652Interleukin-22 [IL-22]
<p>F-652, a first-in-class biological drug, is a recombinant fusion protein consisting of a human interleukin 22 (IL-22) moiety and a human IgG2 Fc moiety. It is produced in Chinese hamster ovary (CHO) cell culture. F-652 exists as a homodimer and has an immunoglobulin-like structure with an IL-22 dimer at the amino (N)-terminal and an Fc fragment at the carboxyl (C)-terminal.</p>
- Alcoholic Hepatitis [AH]
Alcohol-related liver disease (ALD) is a major cause of morbidity and mortality in the world and encompasses a clinical-histologic spectrum of diseases including fatty liver, alcoholic hepatitis (AH), and alcohol-related cirrhosis. AH is a severe and life threatening form of ALD. The prevalence of AH has not been accurately determined, but it is believed to occur in 10% to 35% of heavy drinkers1. AH is an inflammatory condition of the liver caused by heavy alcohol consumption over an extended period. It develops in patients with steatosis and is usually associated with progressive fibrosis. AH is characterized by infiltration of the liver by inflammatory cells and hepatocellular injury. It presents with a syndrome of progressive inflammatory liver injury, including a spectrum of diseases that range from mild injury to severe, life-threatening injury.
Severe AH may be associated with 90-day mortality upwards of 40%.1 There have not been more effective drugs successfully developed since corticosteroids were introduced for the treatment of severe AH in the early 1970s. Moreover, only 40% of patients have a response to standard treatment with steroids.1 Corticosteroids are also contraindicated in the presence of infection, gastrointestinal bleeding, pancreatitis, and viral hepatitis. A recent study of the most commonly used agents in the treatment of AH2 showed benefit with prednisone only at one month and no survival benefit with pentoxifylline. Therefore, development of novel therapeutics to treat ALD, especially AH, remains a tremendous challenge, highlighting a significant unmet need for these patients. Based on the current accumulated knowledge of IL-22 biology, IL-22 is believed to be promising for the treatment of ALD.
- Acute-on-Chronic Liver Failure [ACLF]
Acute-on-chronic liver failure (ACLF) is a recently described entity in the natural history of cirrhosis, defined by acute insult leading to rapid hepatic decompensation, multiple organ failure, and a high risk of short-term mortality (usually less than four weeks). Though there are different diagnostic criteria by various international consortia around the world, in recent years it has been accepted that ACLF defines patients with cirrhosis who are non-electively admitted to the hospital for recent onset ascites, gastrointestinal hemorrhage, newly developed hepatic encephalopathy, bacterial infections, or any combination of these disorders. Three major features characterize this syndrome: it occurs in the context of intense systemic inflammation; it frequently develops in close proximal temporal relationship with pro-inflammatory precipitating events (e.g., infections or alcoholic hepatitis); and it is associated with single or multiple-organ failure.
ACLF is an extraordinarily dynamic syndrome which can either be reversible in a considerable proportion of patients or even completely resolve in up to 50% of cases,3 while in others it may deteriorate to a life-threatening condition due to disease progression in a short period of time. Patients with different etiologies vary in clinical features. The management of ACLF includes etiology-based treatment, controlling and treating complications, providing artificial liver support system, liver transplantation, and so on. Organ functions need to be monitored closely and organ-specific treatment is required to restrict the development of multiorgan failures. ACLF is still a major medical problem around the world, and it poses a major threat to public health due to the high mortality rate.
IL-22 is a potential agent for treating patients with ACLF because it can protect tissue from acute liver injury, inflammation, and infection. Indeed, F-652 therapy promoted liver regeneration, attenuated bacterial infection, improved liver function, and significantly increased the survival rate in ACLF mice.
- Acute Graft Versus Host Disease [aGVHD]
GVHD occurs after allogeneic bone marrow or hematopoietic cell transplantation which are commonly used to treat hematological cancers. GVHD occurs when donor-derived immune cells recognize the transplant recipient (the host) as foreign, thereby initiating an immune reaction and subsequent inflammatory cascade that results in varying degrees of tissue damage and potential organ failure in the transplant recipient. Despite prophylactic treatments with immunosuppressive agents, approximately 50% of transplantation recipients develop GVHD. Approximately 40% and 60% of hematopoietic cell transplantation patients develop GVHD in matched (sibling/related donor) and mismatched (unrelated donor) patients, respectively.
Acute GVHD (aGVHD) and chronic GVHD (cGVHD) remain as major contributors to transplantation-related deaths and the most significant barriers to the success of transplantation. GVHD in association with infection and organ failure contributes approximately 40% of the mortality for transplantation overall. Most GVHD reactions are undesirable and affect multiple organs including skin, liver and gastrointestinal tract.
Although steroids were the first-line treatment for aGVHD in clinical practice for many decades and immuno-suppressants with cytotoxic agents are currently used for prophylaxis and management of GVHD after transplantation, efficacy outcomes and long-term survival in patients remains very challenging. A drug candidate with a novel mechanism of action would have a great potential to improve the current clinical outcome for patients. Mounting evidence from animal and human studies support the potential use of IL-22 as a promising first line therapy for treating aGVHD.
- Necrotizing Enterocolitis [NEC]
Necrotizing enterocolitis (NEC) is an inflammatory intestinal disease characterized by the impairment of the epithelial barrier. NEC primarily affects premature neonates of low birth weight and has a very high morbidity and mortality. It is triggered by an exaggerated inflammatory response resulting in gut barrier dysfunction, intestinal stem cell loss, and impaired mucosal healing, with resultant intestinal necrosis and intestinal perforation in the most extreme cases, requiring surgical intervention. NEC may further lead to systemic inflammation, affecting distant organs such as the brain, and placing affected infants at substantially increased risk for neurodevelopmental delays.
NEC is a leading cause of death in premature infants. This devastating disease occurs in 10% of premature infants with half of these infants requiring surgical removal of the necrotic intestine with an associated mortality rate of 50%.5
NEC is a complex and multifactorial disease, and several factors can increase a newborn’s risk of developing NEC, including prematurity, formula feeding, difficult birth delivery, and an overgrowth of germs in the intestines. However, the precise etiology remains unknown.
Currently, the treatment of NEC includes stopping feedings, parenteral antibiotics, nasogastric decompression, parenteral nutrition, fluid resuscitation, and surgery. However, the available preventative and therapeutic methods for NEC fail to reduce the incidence of NEC and associated morbidity and mortality, which continue to rise.
Recent studies suggest that IL-22 is essential for the maintenance of the gut barrier IL-22 has been shown to play a key role in attenuating intestinal inflammation, maintaining the gut barrier, and is critical for intestinal stem cell-mediated epithelial regeneration. In addition, it has been shown that enhancing mucosal healing and intestinal stem cell regeneration can attenuate NEC in pre-clinical studies. Therefore, it is worth seeking to determine whether recombinant human IL-22-Fc (F-652) administration may prevent and/or treat intestinal inflammation in NEC.